
Ankle Sprains - A factsheet
Who Suffers These and How?
Ankle ligament ruptures usually occur after the ankle twists suddenly, such as when landing awkwardly during sport, stepping off a curb, falling from a height (such as scaffolding or from a truck) or slipping on uneven ground. The most common type happens when the foot rolls inward (an inversion injury), straining the ligaments on the outer side of the ankle. These injuries are common among active adults, manual workers, athletes, but can affect anyone — even during routine daily activities. Sports that involve rapid direction changes (e.g. football, basketball, netball, or trail running) carry the highest risk (1,5,6).
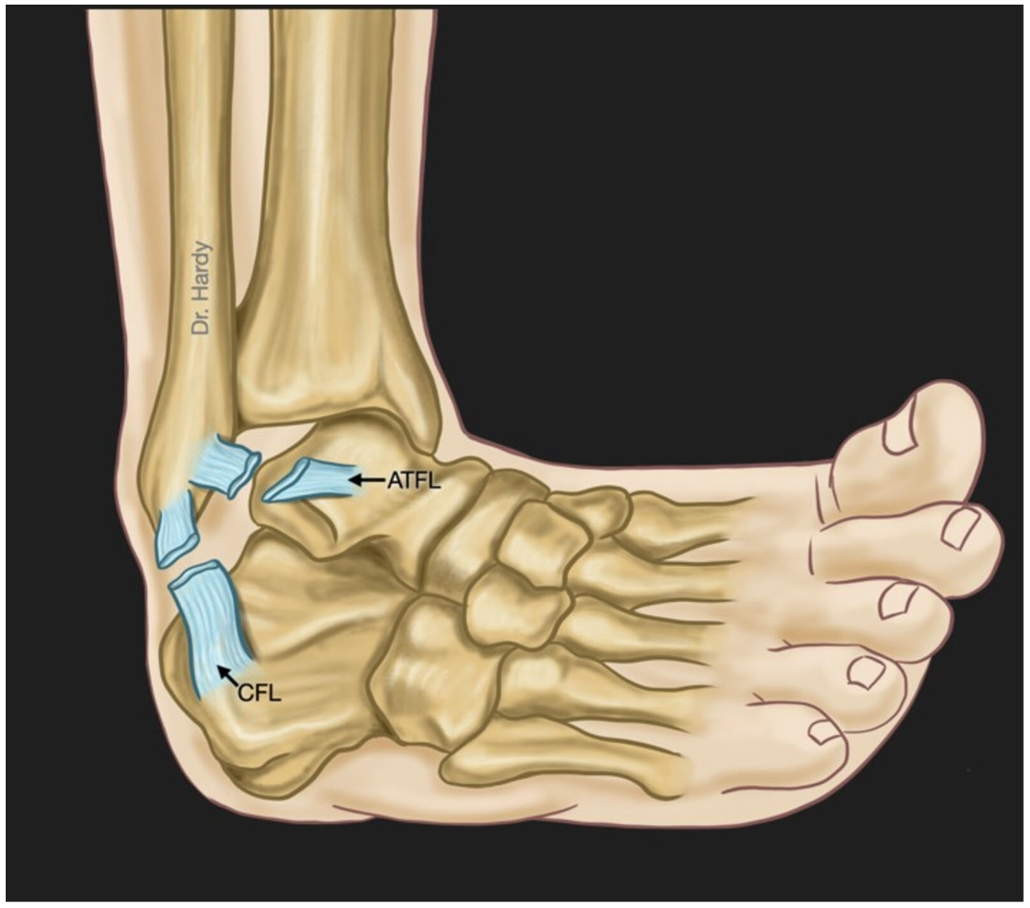
Fig 1. The Anterior talofibular ligament (ATFL) and calcaneofibular ligament (CFL) are the most commonly injured ligaments during a traditional “ankle sprain”.
What Gets Damaged?
The ankle joint is stabilised by several ligaments that connect bones together and keep the joint steady (1):
• Lateral ligaments: The anterior talofibular ligament (ATFL), calcaneofibular ligament (CFL), and posterior talofibular ligament (PTFL) are most often injured when the foot rolls inwards.
• Medial ligament: The deltoid ligament on the inner side is injured far less often.
• Syndesmosis: The strong ligaments between the tibia and fibula can be damaged in “high ankle sprains” (2,3).
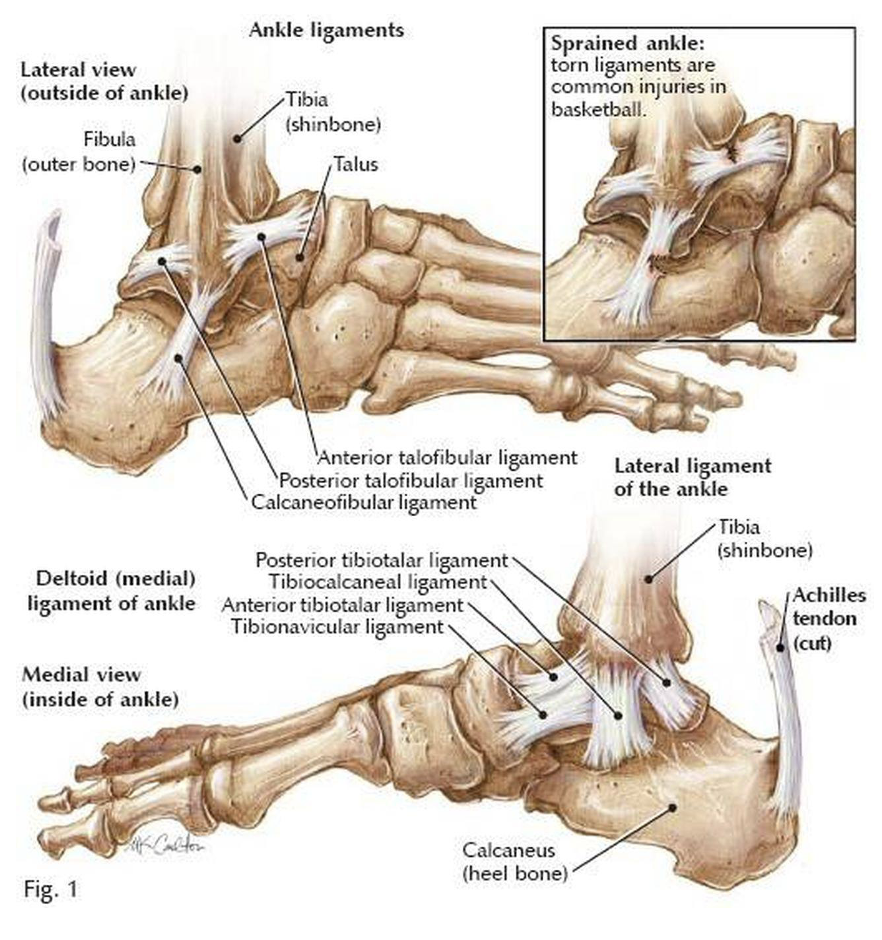
Fig 2. A diagram of the anatomy of the medial and lateral ankle ligaments.
What Is the Initial Treatment (first few weeks)?
Immediate care should follow the R.I.C.E. principle: Rest, Ice, Compression, Elevation Simple pain relief and short-term use of crutches or a supportive boot may be advised. Early, gentle range-of-motion exercises help prevent stiffness once the worst pain and swelling settle.
In most cases, rehabilitation should start within a few days to encourage healing and restore movement. Common early exercises include a focus on: 1. Range of Motion, 2. Strengthening, 3. Balance and Proprioception and 4. Gradual Progression and return to activity. (7,8)
Most cases (up to 90%) improve with a comprehensive rehabilitation program, including (1,3):
Physiotherapy: Focused exercises to strengthen the muscles around the ankle and restore balance.
Bracing or taping: Provides extra support during sport or high-risk activities.
Activity modification: Gradual return to sport with tailored exercises to prevent re-injury.
When to See a Specialist?
You should seek medical review or see an orthopaedic specialist if:
You cannot walk more than a few steps immediately after the injury.
There is significant swelling, bruising, or deformity of the ankle.
Pain remains severe after several days, or you cannot return to normal activities.
The ankle feels unstable or ‘gives way’.
You experience recurrent sprains or ongoing pain after a previous injury.
In particular – Severe pain and/or swelling may indicate injuries to the deltoid ligament and syndesmosis. These can result in a poor outcome for patients and prompt review with a specialist orthopaedic surgeon is recommended (1,4,9).
What Are the Signs and Symptoms of Long-Term Instability?
If the ligaments do not heal properly, some patients develop chronic ankle instability, which may include:
Repeated ‘rolling’ or ‘giving way’ of the ankle, especially on uneven ground.
Persistent pain, swelling, or stiffness.
A feeling that the ankle is weak or unreliable during sport.
Difficulty performing balance or cutting movements.
Occasional catching, clicking, or locking if there is cartilage injury. (1,3)
If you are experiencing these symptoms after you have tried rehabilitation for a period of 10-12 weeks after the initial injury or, you have had multiple severe sprain episodes. Review with a specialist orthopaedic surgeon is recommended to discuss ankle stabilisation surgery.
What Are the Treatment Options for Chronic Instability?
If symptoms persist after physiotherapy, surgical reconstruction may be recommended. For patients that are deemed suitable - Surgery involves tightening or reconstructing the damaged ligaments, sometimes using grafts or internal bracing devices (1). In some cases this can be done via keyhole surgery (arthroscopic), but your surgeon will discuss this with you.
The outcomes of ankle stabilisation surgery in these cases are excellent, with up to 95% of patients have a successful outcome.
Chronic ankle instability, apart from being debilitating and affecting quality of life. Is the most common cause of ankle osteoarthritis (up to 90%), which may require reconstructive or joint replacement surgery at a young age (10,11).
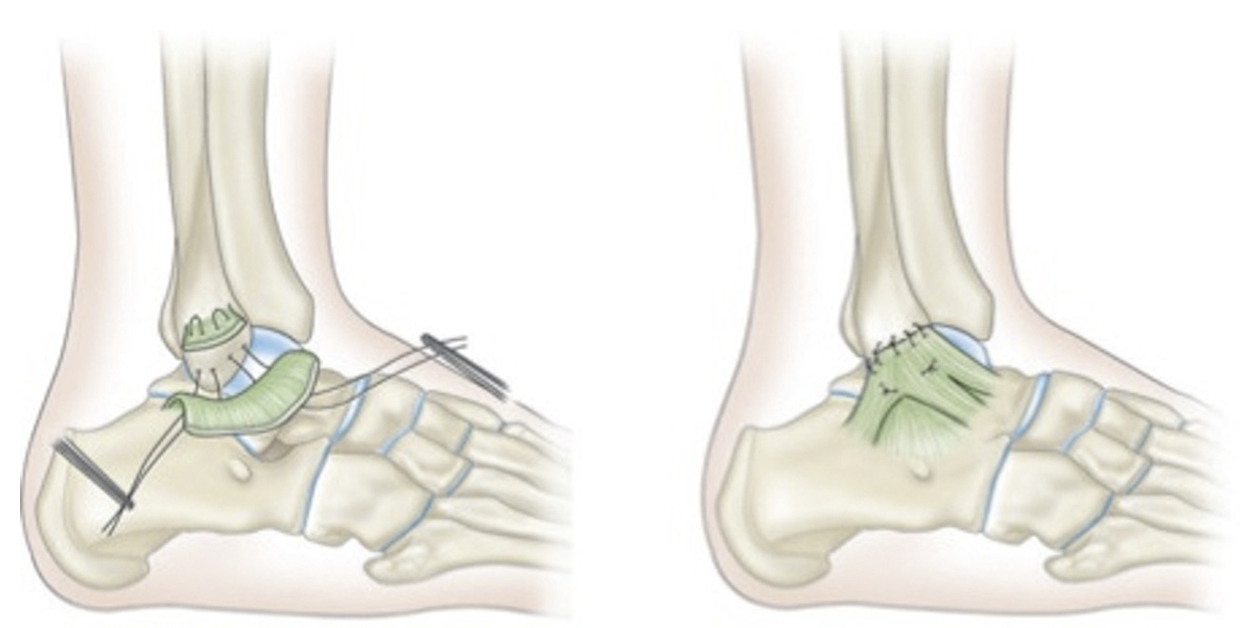
Fig 3. Diagrammatic representation of a type of ankle lateral ligament reconstruction.
Summary
Ankle ligament ruptures are common injuries, especially in active people. With early recognition, appropriate initial care, and a guided rehabilitation plan, most individuals make a full recovery. Persistent pain or instability should always be assessed by a specialist, as timely treatment can prevent long-term ankle problems and allow a safe return to sport and daily activity.
References
1. C. De Cesar Netto, M. Lalevee, K.A.M. Carvalho, K. Dibbern, E.I. Ferkel, V. Valderrabano, A.L. Godoy-Santos, A. Ehret, N.S.B. Mansur, Multiligament Ankle Instability Following Rotational Ankle Injuries: A Prospective Cohort Study, Foot & Ankle Orthopaedics 8 (2023) 2473011423S00354. https://doi.org/10.1177/2473011423S00354.
2. E.H. Park, C. De Cesar Netto, J. Fritz, MRI in Acute Ankle Sprains, Foot and Ankle Clinics 28 (2023) 231–264.https://doi.org/10.1016/j.fcl.2023.01.011.
3. Chandran, R.E. Moffit, A.F. DeJong Lempke, A.J. Boltz, A.S. Alexander, H.J. Robison, Z.Y. Kerr, C.L. Collins, E.A. Wikstrom, Epidemiology of Lateral Ligament Complex Tears of the Ankle in National Collegiate Athletic Association (NCAA) Sports: 2014-15 Through 2018-19., Am J Sports Med 51 (2023). https://doi.org/10.1177/03635465221138281.
4. B.R. Waterman, P.J. Belmont, K.L. Cameron, S.J. Svoboda, C.J. Alitz, B.D. Owens, Risk Factors for Syndesmotic and Medial Ankle Sprain: Role of Sex, Sport, and Level of Competition, Am J Sports Med 39 (2011) 992–998. https://doi.org/10.1177/0363546510391462.
5. N. Kofotolis, E. Kellis, Ankle sprain injuries: a 2-year prospective cohort study in female Greek professional basketball players, J Athl Train 42 (2007) 388–394.
6. D.T.-P. Fong, Y. Hong, L.-K. Chan, P.S.-H. Yung, K.-M. Chan, A systematic review on ankle injury and ankle sprain in sports, Sports Med 37 (2007) 73–94. https://doi.org/10.2165/00007256-200737010-00006.
7. B.D. Beynnon, P.M. Vacek, D. Murphy, D. Alosa, D. Paller, First-time inversion ankle ligament trauma: the effects of sex, level of competition, and sport on the incidence of injury., Am J Sports Med 33 (2005). https://doi.org/10.1177/0363546505275490.
8. E. Giza, C. Fuller, A. Junge, J. Dvorak, Mechanisms of Foot and Ankle Injuries in Soccer, Am J Sports Med 31 (2003) 550–554. https://doi.org/10.1177/03635465030310041201.
9. Beynnon B.D., Renstrom P.A., Alosa D.M., Baumhauer J.F., Vacek P.M., Ankle ligament injury risk factors: A prospective study of college athletes, Journal of Orthopaedic Research 19 (2001). https://doi.org/10.1016/s0736-0266%25252800%25252990004-4.
10. M. Herrera-Pérez, D. González-Martín, M. Vallejo-Márquez, A.L. Godoy-Santos, V. Valderrabano, S. Tejero, Ankle Osteoarthritis Aetiology, JCM 10 (2021) 4489. https://doi.org/10.3390/jcm10194489.
11. V. Valderrabano, M. Horisberger, I. Russell, H. Dougall, B. Hintermann, Etiology of Ankle Osteoarthritis, Clinical Orthopaedics & Related Research 467 (2009) 1800–1806. https://doi.org/10.1007/s11999-008-0543-6.