
Base of 5th Metatarsal Fractures: What You Need to Know
A sudden snap when you roll your ankle, or a nagging ache on the outer edge of your foot that won't settle — both can signal a base of 5th metatarsal fracture. This is one of the most common foot fractures I see in my Melbourne practice. The critical thing to understand is that not all of these fractures are the same, and treatment that is appropriate for one type can be entirely wrong for another.
Anatomy and Why Blood Supply Matters
The fifth metatarsal runs along the outer border of the foot. Several structures attach at its base: the peroneus brevis tendon, the plantar fascia, and the abductor digiti minimi. The bone's main blood supply enters the shaft through a blood vessel a short distance from the base. This leaves the metadiaphyseal junction — the area between the base and shaft — relatively poorly vascularised from both sides. It is exactly this zone that is most prone to non-union.
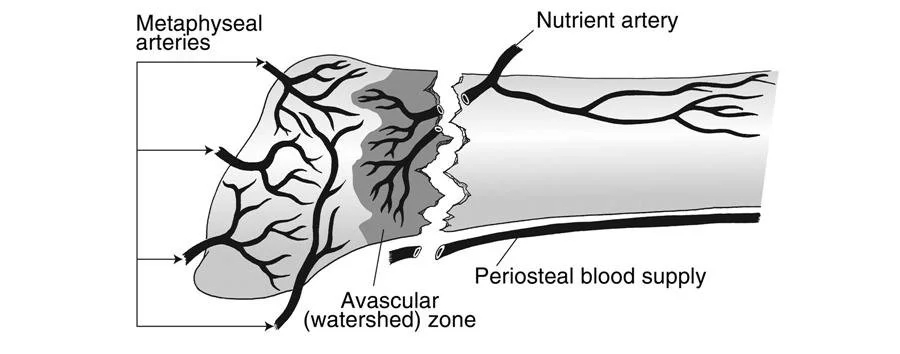
Figure 1: the blood supply to the base of 5th metatarsal
Zone 1, Zone 2 and Zone 3: Why Location Changes Everything
The Lawrence and Botte classification divides the base of the 5th metatarsal into three zones, each with a different injury pattern and prognosis.
Zone 1 — Avulsion Fracture
The most common type. A sudden ankle roll causes the peroneus brevis tendon to pull a bony fragment from the base of the bone. Blood supply is good here and the vast majority heal well with a boot and protected weight-bearing over 4–6 weeks, without surgery.
Zone 2 — The Jones Fracture
The Jones fracture sits at the poorly vascularised metadiaphyseal junction. It typically results from a single forceful event — an awkward landing, a pivot, or a tackle — and carries a meaningful risk of non-union and re-fracture, particularly in athletes who return to sport too soon. This is the fracture I see most commonly in AFL, soccer and basketball players.
Zone 3 — Diaphyseal Stress Fracture
Zone 3 fractures occur further along the shaft and are almost always stress fractures, developing over weeks of repetitive overload rather than a single incident.
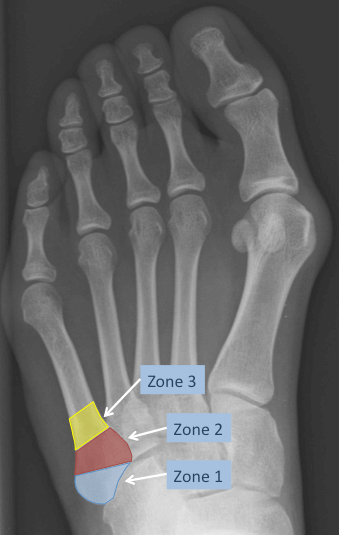
Figure 2: a dorsoplantar X-ray of the left foot demonstrating the aforementioned “zones” of injury in base of 5th metatarsal fractures
Stress Fractures in Athletes
Stress fractures of the 5th metatarsal are a particular concern in runners, basketballers, footballers and dancers. Early symptoms are easy to dismiss — a dull ache on the outer midfoot that worsens with training and eases with rest. Plain X-rays are often normal in the early stages; MRI is the investigation of choice, detecting bone marrow oedema before a fracture line is visible. CT is used for surgical planning once a fracture is confirmed.
Why a High-Arched (Cavovarus) Foot Increases Risk
A cavovarus foot — high medial arch, heel tilting inward — transfers disproportionate load through the outer border of the foot with every step. This substantially increases the risk of 5th metatarsal stress fractures, and more importantly, undermines healing after treatment. Every patient I see with a Jones fracture or stress fracture is assessed for an underlying cavovarus deformity. If present, addressing the alignment — with orthotics or, in significant cases, a corrective osteotomy — is an essential part of preventing recurrence.
When Is Surgery Needed?
Non-Surgical Management
Non-surgical treatment is appropriate for Zone 1 avulsion fractures in most patients, undisplaced Zone 2 fractures in low-demand individuals, and early stress fractures detected at the bone marrow oedema stage. A period of weight-bearing in a boot (typically 4-6 weeks), followed by gradual loading and imaging to confirm healing, is the standard approach. The key risk is a non-union rate of up to 25% in some series for Jones fractures (zone 2) managed non-surgically. For this reason many of my patients opt for surgical intervention early.
Intramedullary Screw Fixation
For competitive athletes and high-demand patients, intramedullary screw fixation is the standard surgical treatment for Zone 2 Jones fractures and many Zone 3 stress fractures. Through a small incision at the base of the bone, a screw is placed down the canal under X-ray guidance to compress the fracture. It is performed as a day surgery procedure. The benefits are significant: lower non-union rate, earlier weight-bearing, and a return to sport at 8–12 weeks compared with 4–5 months or longer with conservative management. Screw sizing matters — I select larger diameter screws (typically 4.5–5.5 mm) based on canal diameter measured on pre-operative CT.

Figure 3: intramedullary screw fixation for a base of 5th metatarsal fracture - in this case a zone 2 (Jones) fracture
Intramedullary Rod Fixation
At Melbourne Orthopaedic Group we treat many athletes, and over many years my senior mentor and colleague David Young has been treating athletes with stress fractures using an operation he pioneered and refined using a specialised 5th Metatarsal rod. This is our operation of choice in the young athlete who has developed a stress fracture of their 5th Metatarsal. You’d be surprised some of the famous names running around with these special DY Rods in their 5th Metatarsal bones.
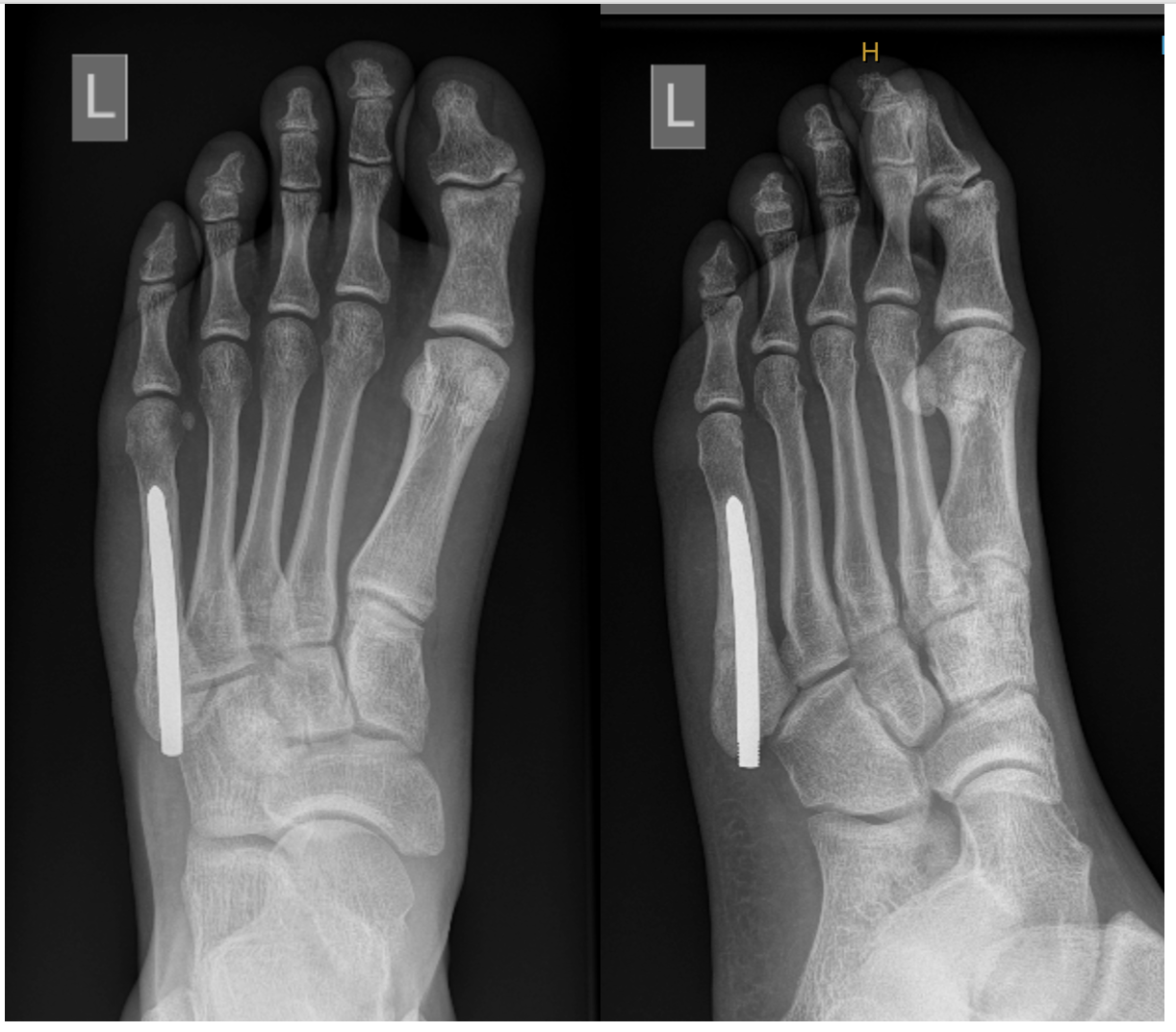
Figure 4: The DY Rod used for fixation of 5th Metatarsal stress fractures in athletes. This operation was developed and refined by my senior colleague and mentor Mr David Young.
Plating and Bone Grafting for Non-Union
When a fracture fails to heal — a non-union — more complex reconstruction is required. This involves surgical debridement of the non-union site, bone grafting (typically harvested from the iliac crest in my practice – the bony part of the hip) to stimulate healing, and stable fixation with either a larger intramedullary screw or a low-profile lateral plate. In patients with cavovarus alignment, deformity correction at the same time significantly improves the chance of successful union.
Summary
Base of 5th metatarsal fractures are common but require accurate assessment and therefore classification.
· Zone 1 avulsion fractures reliably heal without surgery. This is the majority of fractures.
· Zone 2 Jones fractures carry a real non-union risk and are best treated surgically in select patients.
· Zone 3 Stress fractures — in athletes or those with a cavovarus foot — need careful assessment to identify and address the underlying cause.
· For fractures that fail to heal, plating and bone grafting offers a pathway to union.
If you have sustained a fracture to the outer border of your foot, or have a 5th metatarsal stress fracture that is not settling with rest, a surgical opinion is often recommended.
Book an appointment: (03) 9124 7960 | talia.admin@mog.com.au
References
1. Lawrence SJ, Botte MJ. Jones' fractures and related fractures of the proximal fifth metatarsal. Foot Ankle. 1993;14(6):358–365.
2. Mologne TS et al. Early screw fixation versus casting in the treatment of acute Jones fractures. Am J Sports Med. 2005;33(7):970–975.
3. Porter DA et al. Fifth metatarsal Jones fracture fixation with a 4.5-mm cannulated stainless steel screw in the competitive and recreational athlete. Am J Sports Med. 2005;33(5):726–733.
4. Ekstrand J, van Dijk CN. Fifth metatarsal fractures among male professional footballers: a potential career-ending disease. Br J Sports Med. 2013;47(12):754–758.
5. Vaz S et al. 5th metatarsal stress fractures in athletes with cavovarus foot: importance of foot alignment assessment. Foot Ankle Surg. 2019;25(4):546–552.