
Modern Ankle Fracture Treatment in Melbourne: Surgery That Gets You Back on Your Feet Sooner
Ankle fractures are among the most common injuries that bring people to an orthopaedic surgeon. A slip on the stairs, a misjudged step off a kerb, a tackle on the football field — and suddenly the joint that carries your entire body weight is broken, swollen and unable to take a step. The good news is that ankle fracture surgery has changed enormously over the last decade. Modern techniques mean stronger fixation, smaller incisions and a faster, more confident return to walking.
This article explains how ankle fractures are managed today, the techniques and technologies a I use as part of my practice at Melbourne Orthopaedic Group and why being treated by a subspecialist could make a measurable difference to your rehabilitation and recovery.
What Is an Ankle Fracture?
An ankle fracture is a break in one or more of the bones that form the ankle joint — the fibula (lateral malleolus), the tibia (medial and posterior malleolus), or the talus. Fractures are graded by the level of the fibular break (the Weber classification — A, B, or C) and by whether the joint remains stable when the foot is loaded. Most ankle fractures cause immediate pain, swelling, bruising and an inability to weight bear. X-rays confirm the diagnosis, and a CT scan is sometimes required to plan surgery for more complex injury patterns.
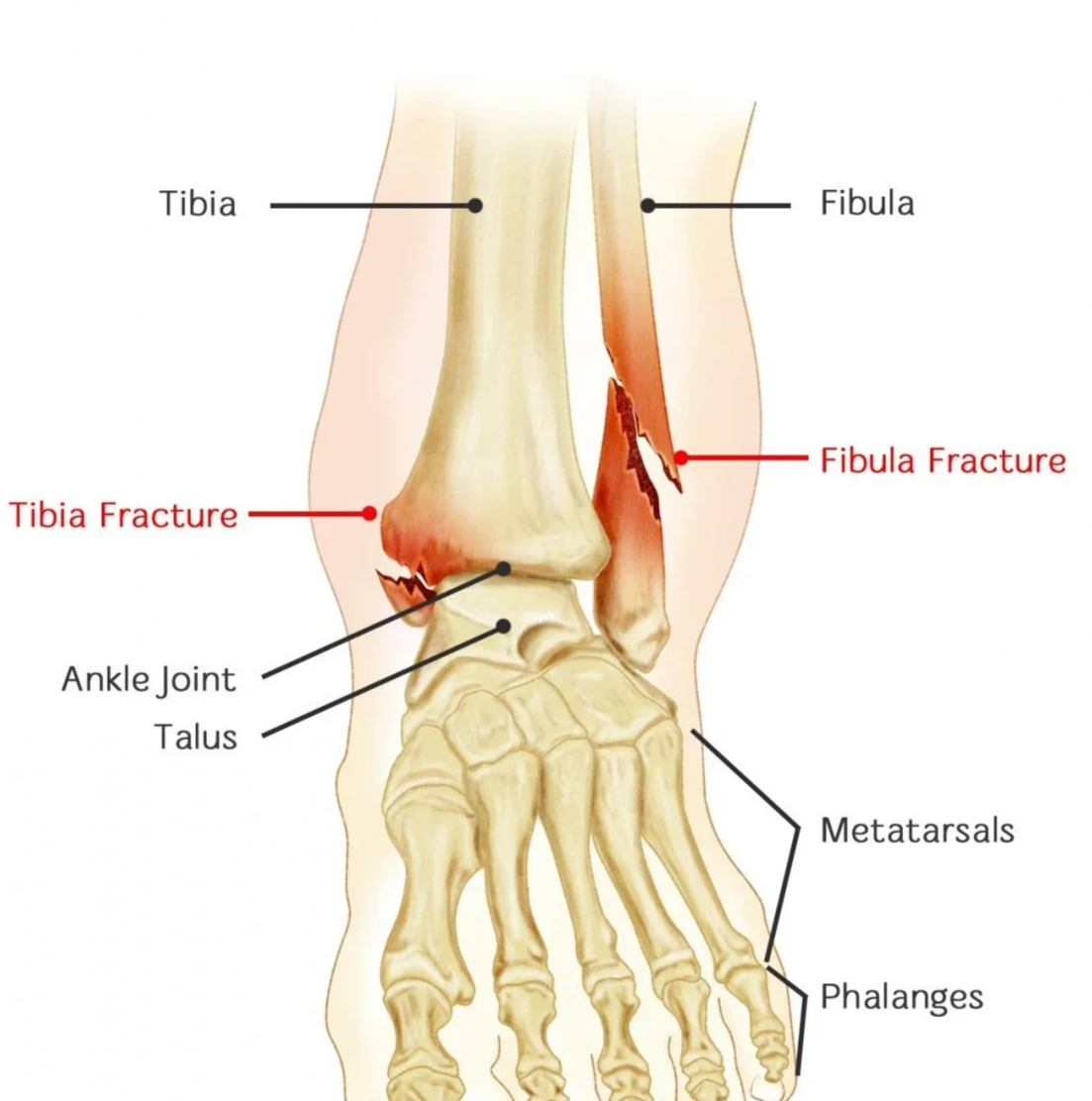
Diagram representing typical pattern of bimalleolar ankle fracture
When Does an Ankle Fracture Need Surgery?
Stable, well-aligned fractures often heal without surgery in a moonboot or cast. In Unstable fractures — typically those with injuries on both sides of the joint, significant displacement, or disruption of the syndesmosis (the ligaments holding the tibia and fibula together) — I typically recommend surgical fixation to restore the precise alignment of the tibia and fibular bones and the joint surface. Even a 1–2 mm shift in the joint can dramatically increase the risk of post-traumatic ankle arthritis years later, which is why anatomical reduction matters.
Modern Ankle Fracture Surgery: What Has Changed
Mr Adrian Talia is a fellowship-trained foot and ankle subspecialist with extensive experience in ankle fracture fixation. His Melbourne practice uses the latest implants and techniques to deliver a more durable repair and a faster, more comfortable recovery.
Anatomical Locking Plates
Today's pre-contoured anatomical locking plates hug the shape of the fibula and lock the screws into the plate, creating a much stronger fixed-angle construct than older one-third tubular plates. This stability allows surgeons to confidently move and load the ankle earlier in recovery.

Modern anatomical locking plate fixation of increasing severity from left to right
Intramedullary Nails
In older patients with thin skin and osteoporotic bone, traditional plates can sometimes fail or cause wound problems. A fibular nail is inserted through a small incision at the tip of the fibula and slides down inside the bone, achieving stable fixation with minimal soft-tissue dissection. Mr Talia has a particular research interest in nail fixation in the elderly, including the use of fibular nailing and tibiotalocalcaneal (TTC) nails for the most fragile injuries.
Dynamic Syndesmosis Stabilisation
When the syndesmosis ligaments are torn, they must be held while they heal. The traditional rigid screw often required a second operation to remove it. Modern flexible suture-button devices allow natural micromotion between the tibia and fibula, lower the rate of malreduction and rarely need to be taken out. Published research work on flexible suture-button devices for ankle fracture stabilisation demonstrate superior outcomes and lower re-operation rates compared with traditional screw fixation of the syndesmosis (1).
Nanoneedle Arthroscopy with the NanoScope
A hidden problem in many ankle fractures is damage to the cartilage inside the joint — an osteochondral injury — which is missed on standard X-rays and even some MRIs. Mr Talia uses the NanoScope which is a 1.9 mm chip-on-tip arthroscope no thicker than a needle that can be placed into the ankle through tiny puncture incisions at the time of fracture fixation. This lets Mr Talia confirm anatomical reduction of the joint from inside the ankle, identify and treat cartilage injuries in the same operation, deliver chondroprotective treatments where required, and give patients a clearer prognosis for long-term joint health. Combining fracture fixation with nano-arthroscopy in a single anaesthetic may addresses problems that could otherwise drive arthritis years later.
Why Early Weight-Bearing Matters: The INWN Trial
For decades, the standard advice after ankle fracture surgery was six weeks of non-weight-bearing in a plaster cast. New evidence has overturned that paradigm. Amongst others, The INWN trial — a multicentre, pragmatic randomised controlled study published in the Journal of Bone and Joint Surgery in 2025 — compared immediate protected weight-bearing in a walking boot from day one against six weeks of non-weight-bearing in a cast (2).
The results were unequivocal. Patients allowed to walk immediately after fixation of their ankle fracture had better functional outcomes, returned to work earlier, and had no increase in complications. The trial provides Level I evidence that early weight-bearing is safer, faster and more effective.
This evidence aligns with how Mr Talia has been treating ankle fractures for some time. The combination of stronger locking-plate or fibular-nail constructs, dynamic syndesmosis fixation, and arthroscopic confirmation of joint reduction creates a repair that is robust enough to load early. Most patients are walking in a moonboot as soon as their wounds have healed, starting physiotherapy in the first weeks, and aiming to be back into normal shoes by six to eight weeks.
Why See a Foot and Ankle Subspecialist
Ankle fractures are common, but every fracture pattern is different. A foot and ankle subspecialist sees these injuries every week, knows which fixation suits which bone, and is comfortable using the full armamentarium of fixation options — locking plates, fibular nails, suture-button syndesmosis fixation, anterior inferior tibiofibular ligament internal brace augmentation and nano-arthroscopy — rather than defaulting to a single technique for all patients.
Mr Adrian Talia is a Melbourne-based orthopaedic surgeon with subspecialty fellowship training in trauma surgery from Western Health; as well as foot and ankle surgery from the Nuffield Orthopaedic Centre, Oxford UK and Swiss Ortho Center, Basel Switzerland. He treats acute ankle fractures at Melbourne Orthopaedic Group and The Avenue Hospital, as well as public practice at Western Health with active research interests in fibular and TTC nail fixation and flexible suture-button stabilisation and AITFL internal brace augmentation.
Book a Consultation
If you or a patient under your care has sustained an ankle fracture, early subspecialty review can make a meaningful difference to the long-term outcome. Visit adriantalia.com.au or phone 03 9124 7960 to discuss.
Referring practitioners can be passed Adrian’s contact details directly to discuss timely care of their patient.
Ræder BW, Figved W, Madsen JE, et al. Better outcome for suture button compared with single syndesmotic screw for syndesmosis injury: five-year results of a randomized controlled trial. The Bone & Joint Journal 2020; 102-B: 212–219.
Khojaly R, Rowan FE, Shah V, et al. Immediate Weight-Bearing Compared with Non-Weight-Bearing After Operative Ankle Fracture Fixation: Results of the INWN Pragmatic, Randomized, Multicenter Trial. Journal of Bone and Joint Surgery 2025; 107: 1423–1438.