
Repairing the Deltoid Ligament in Ankle Fractures: A Shift Towards Faster, More Stable Recovery
An ankle fracture is rarely just a broken bone. In more severe injuries — typically those involving fractures on both sides of the ankle, or with disruption of the syndesmosis, the ligaments holding the tibia and fibula together — there is frequently a concurrent rupture of the deltoid ligament on the inner side of the ankle. For a long time, the deltoid was left to heal on its own. New evidence, and a shift in how modern foot and ankle surgeons approach these injuries, tells a different story.
What Is the Deltoid Ligament?
The deltoid ligament is a broad, fan-shaped structure on the medial (inner) side of the ankle. It runs from the medial malleolus — the bony bump on the inside of your ankle — down to the talus and calcaneus (heel bone). It has two layers: a superficial layer that resists valgus (outward) stress, and a deep layer that controls external rotation of the talus within the ankle socket.
Critically, the deltoid is not just a medial stabiliser. Cadaveric research has demonstrated that it plays a key role in syndesmotic stability. When both the anterior inferior tibiofibular ligament (AITFL) and the deltoid are disrupted, the ankle mortise — the socket that holds the ankle joint together — becomes significantly more unstable than when either ligament is injured alone. In other words, the deltoid is part of the global stabilising system of the ankle, not just a secondary structure on the inside.
The Traditional Approach: Fix the Fibula, Leave the Deltoid
For decades, the standard surgical approach to complex ankle fractures with both syndesmotic injury and deltoid rupture was to fix the fibular fracture with a plate, then stabilise the syndesmosis with a rigid trans-syndesmotic screw. The deltoid was left unrepaired on the assumption it would heal indirectly and that conservative management was adequate.
The problem with syndesmotic screws is well-documented. Malreduction, screw breakage, restricted ankle motion, and the frequent need for a second operation to remove the hardware have driven surgeons to search for better alternatives. More flexible suture-button tightrope devices have improved on screws in many respects, but the question of the deltoid has remained.
Schematic for an anatomic deltoid reconstruction.
Reproduced from: Olory B, Agostinone P, Hantouly AT, et al. Four‐bundle anatomic deltoid ligament reconstruction: Surgical technique. J exp orthop 2025; 12: e70279.
The Case for Deltoid Repair and Augmentation
A growing body of literature has challenged the assumption that the deltoid can simply be left alone. A recent prospective randomised controlled trial published in the journal Injury (Li et al., 2026) provides the strongest evidence yet that deltoid ligament augmentation (DLA) can replace syndesmotic fixation altogether in selected cases — and that when it does, patients recover faster.
The study recruited 60 patients with acute ankle fractures involving both syndesmotic instability and deltoid rupture — the most complex and unstable fracture pattern. After fibular fixation, patients were randomised to either deltoid ligament augmentation or standard trans-syndesmotic screw fixation. The primary outcome was the American Orthopaedic Foot and Ankle Society (AOFAS) score at one year.
At 12 months, both groups achieved equivalent functional outcomes — the deltoid augmentation was non-inferior to screw fixation in terms of long-term clinical results. But the early recovery picture was markedly different. Patients in the DLA group experienced:
• Significantly earlier partial weight-bearing
• Earlier full weight-bearing
• Faster return to work and preinjury-level activity
• Better ankle range of motion at 3 months (particularly dorsiflexion)
• Avoidance of a second operation to remove syndesmotic hardware
The mechanism is logical: by repairing the medial column directly, the syndesmosis is reduced indirectly through restoration of the ankle mortise’s own stability. This avoids the need for rigid hardware that restricts ankle motion and carries the risk of breakage under load.
How Is Deltoid Ligament Augmentation Performed?
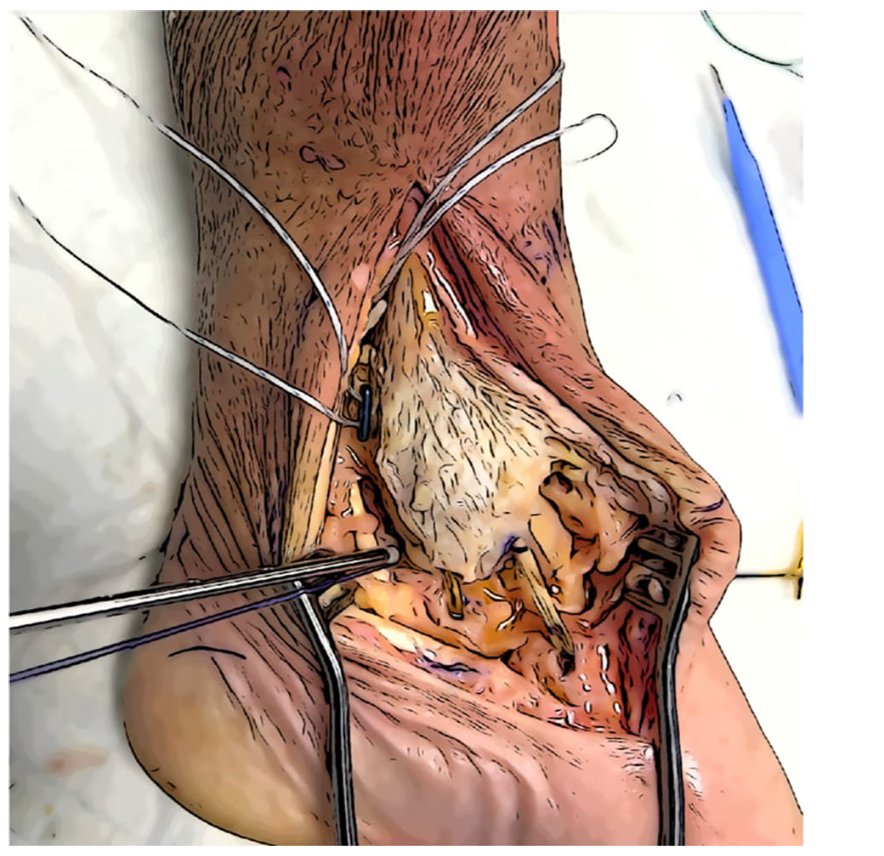
In the technique described by Li et al., after the fibular fracture is fixed and syndesmotic instability is confirmed under intraoperative stress testing, a curved medial incision is made. The deep deltoid — which is difficult to suture directly due to the confined space medially — is reconstructed using a suture anchor placed into the talus, with the suture threads passed through bone tunnels in the medial malleolus and tied down securely. The superficial deltoid layer is repaired directly where possible.
This bone-to-bone augmentation technique restores the primary medial stabiliser of the ankle, and the native congruency of the mortise then holds the syndesmosis in correct alignment without the need for trans-syndesmotic hardware.
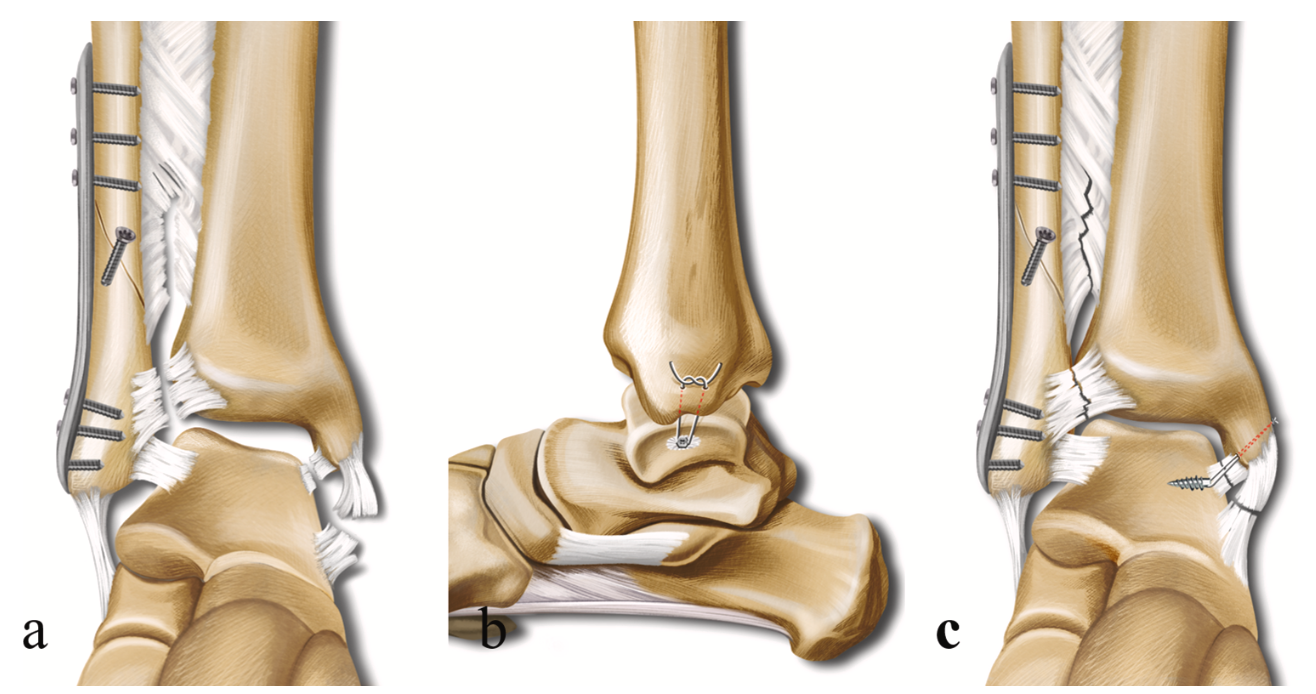
Deltoid augmentation in ankle fracture schematic. with both syndesmotic diastasis and DL rupture. After the reduction and fixation of the fibular fracture, ankle congruity was still not conducted because of both syndesmosis and medial column instability (a). After DLA with a suture anchor, the stability of the medial column was restored, and syndesmosis was reduced indirectly (b, c).
Reproduced from: Li T, Sun Z, Sun X, et al. Deltoid ligament augmentation replacing syndesmotic fixation for the treatment of ankle fractures: a prospective randomized controlled study. Injury 2026; 57: 112922.
What This Means in Modern Ankle Fracture Surgery
We see these injuries regularly at Melbourne Orthopaedic Group and in my public post at Western Health. Complex ankle fractures with deltoid rupture and syndesmotic diastasis represent one of the most unstable patterns we manage, and the question of how to address the medial-side injury is one I think carefully about in each case.
The critical thing to understand is that leaving the deltoid unrepaired in these high-grade injuries means accepting medial-column instability and relying entirely on syndesmotic hardware to maintain the mortise. When that hardware is a rigid screw, the patient cannot safely weight-bear until it is removed — typically at 10 to 12 weeks. That’s three months of restricted function, with a second operation, before rehabilitation can truly begin.
In active individuals — and certainly in those who need to return to work or sport — I favour a repair and augment approach to the deltoid where the anatomy is suitable. Addressing the deltoid directly means the syndesmosis can be reduced indirectly and held there by the joint’s own reconstructed ligaments rather than by metal hardware. It creates a repair that is robust enough to load early, and it avoids the risks and inconvenience of implant removal.
This aligns with the broader direction of modern foot and ankle surgery: move away from rigid, hardware-dependent fixation and towards anatomical ligament restoration that respects the biology and mechanics of the joint.
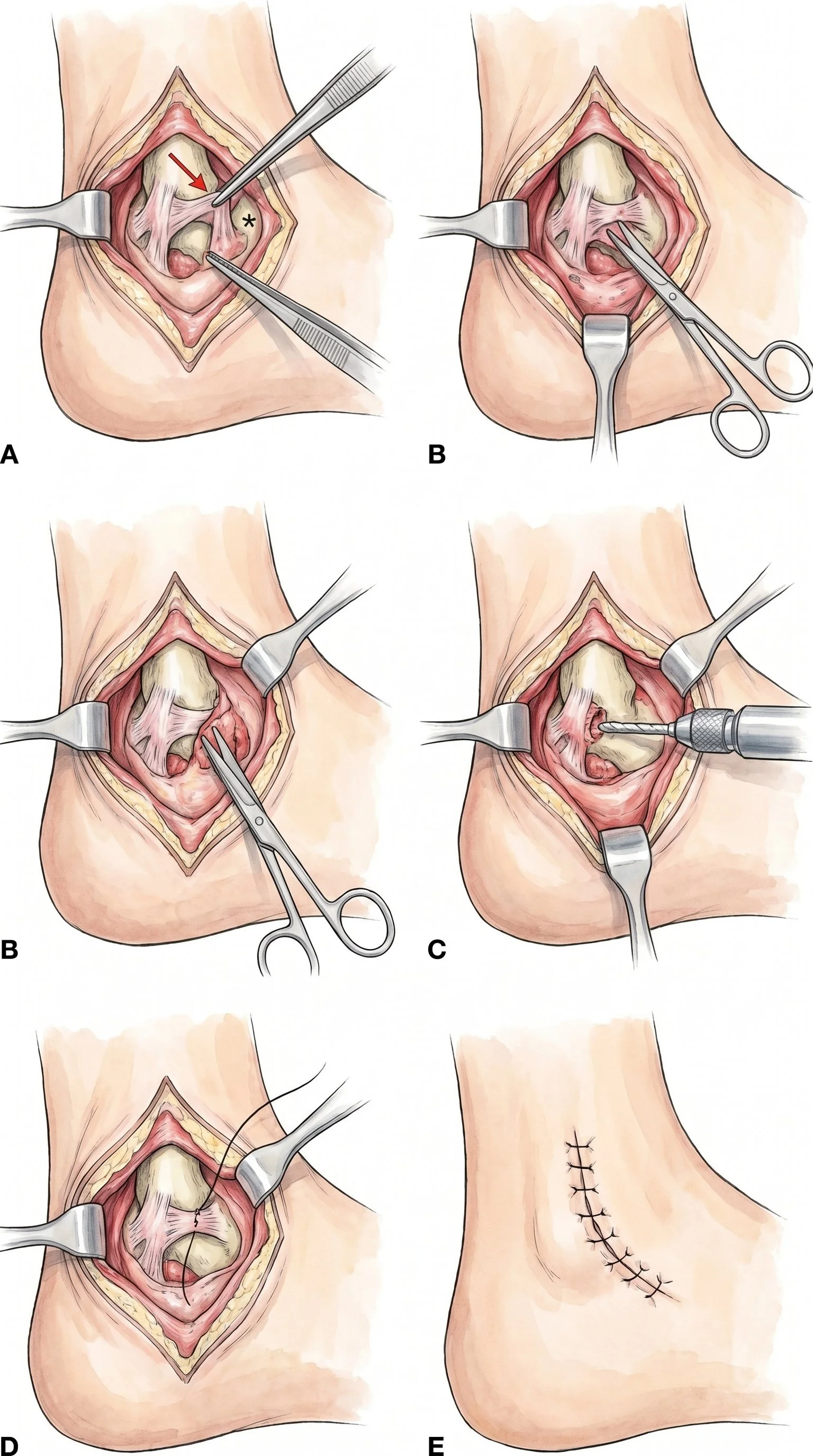
Deltoid ligament repair schematic
Recovery After Deltoid Ligament Repair
A general recovery framework for my patients after deltoid ligament augmentation in conjunction with ankle fracture fixation:
• Weeks 0–2: Short leg splint, elevation, gentle toe and foot exercises.
• Weeks 2–6: Progressive weight-bearing in a moonboot as tolerated. Physiotherapy begins — range of motion, swelling management, early muscle activation.
• Weeks 6–12: Transition to normal footwear. Return to low-impact activity. Functional strengthening and balance work.
• 3–6 months: Return to full activity for most patients, depending on fracture complexity and individual factors. No second operation required.
Summary
The deltoid ligament is the primary medial stabiliser of the ankle and plays a direct role in syndesmotic stability. In complex ankle fractures with both deltoid rupture and syndesmotic diastasis, direct repair and augmentation of the deltoid offers equivalent long-term outcomes to syndesmotic screw fixation, with a faster early recovery, earlier weight-bearing, and no need for hardware removal. This approach reflects the direction modern foot and ankle surgery is heading: anatomical reconstruction, early rehabilitation, and fewer operations.
If you or a patient under your care has sustained a complex ankle fracture, early subspecialty review can make a meaningful difference to the outcome. I would be happy to see you of course, and urgent treatment can always be accomodated.
Book an appointment: (03) 9124 7960 | talia.admin@mog.com.au
References
1. Li T, Sun Z, Sun X, Li C, Fei H, Gong M, Wu X, Jiang X. Deltoid ligament augmentation replacing syndesmotic fixation for the treatment of ankle fractures: a prospective randomized controlled study. Injury.2026;57:112922. doi:10.1016/j.injury.2025.112922
2. Massri-Pugin J, Lubberts B, Vopat BG, et al. Role of the deltoid ligament in syndesmotic instability. Foot Ankle Int. 2018;39(5):598–603.
3. Schottel PC, Baxter J, Gilbert S, et al. Anatomic ligament repair restores ankle and syndesmotic rotational stability as much as syndesmotic screw fixation. J Orthop Trauma. 2016;30(1):e36–40.
4. James M, Dodd A. Management of deltoid ligament injuries in acute ankle fracture: a systematic review. Can J Surg. 2022;65:E9–15.