
Early Weight Bearing After Total Ankle Replacement: What the Latest Research Tells Us
One of the most common questions patients ask before total ankle replacement surgery is: how soon can I walk again?
Traditionally, the answer has been: not for a while. Post-operative protocols have historically kept patients completely off the operated foot for six to twelve weeks — the thinking being to let the implant settle and protect the wound before loading the joint.
For many years at Melbourne Orthopaedic Group, we have taken a different approach. For patients undergoing INBONE (stemmed) total ankle replacement, we allow weight bearing in a CAM boot as soon as the surgical incisions have healed — typically around the two-three week mark. Getting patients on their feet earlier minimises muscle wasting, reduces the bone loss (osteopaenia) that comes with prolonged immobility, and improves functional outcomes. It is always gratifying when the science catches up to clinical practice — and a study published in 2026 in Foot & Ankle International now provides the first direct comparative evidence that early weight bearing after ankle replacement is not only safe, but actively beneficial.
What Did the Study Examine?
Nguyen and colleagues from Chicago, USA examined 77 patients who underwent primary total ankle replacement using the INBONE II prosthesis — the same implant we use for select patients at Melbourne Orthopaedic Group. Patients were divided into two groups: those who began weight bearing at three weeks (50 patients) and those who remained non-weight-bearing until six weeks (27 patients). All patients were followed for a minimum of two years.
The researchers measured ankle range of motion — how far the ankle bends up and down — at regular intervals using standardised X-rays, and carefully tracked all complications, from minor wound issues through to implant failure.
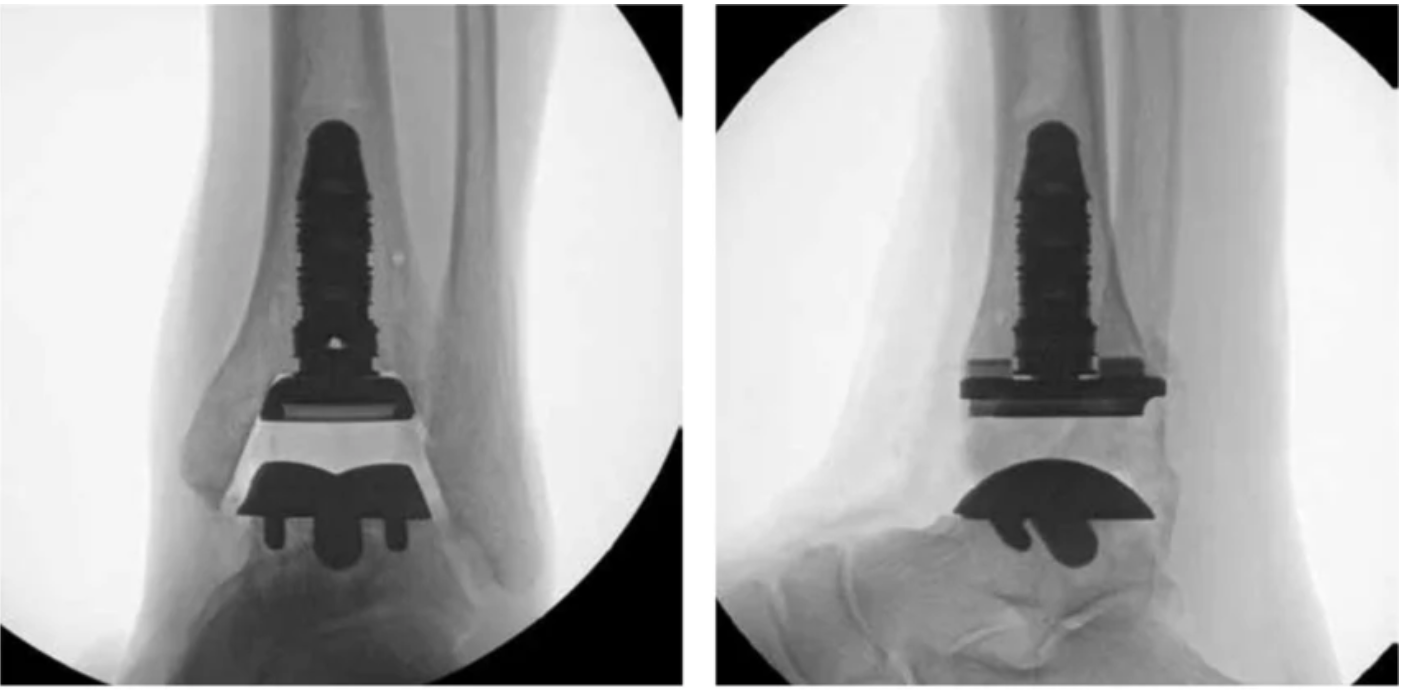
X-ray images of the INBONE II implant Total Ankle Replacement system. Intra-operative anterior-posterior and lateral fluoroscopic images of the ankle with INBONE II implant system. (Image courtesy of Wright Medical Technology, Inc., Memphis, TN, US)
What Did the Results Show?
The results favoured earlier mobilisation.
In the three-week group, ankle range of motion had recovered to pre-operative levels by six weeks, and by six months it had exceeded pre-operative values. This improvement was sustained at one and two years. The six-week group, by contrast, did not achieve a statistically significant improvement in ankle movement beyond their pre-operative baseline at any point from three months onwards.
When compared head-to-head, the three-week group had significantly greater ankle movement at six weeks, six months, one year, and two years — even after adjusting for differences in age, body weight, and pre-operative ankle motion.
Was It Safe?
The answer is clearly yes. Complication rates were 19% in the three-week group and 16% in the six-week group — not a meaningful difference. Reoperation rates were 6.0% versus 7.4% respectively, and implant survivorship was 98% versus 100%. None of these differences were statistically significant.
Notably, the three-week group was nearly seven years older on average (67.8 versus 61.1 years) — meaning the earlier weight-bearing patients were the more medically vulnerable cohort, yet experienced no greater risk. This matters, because older patients are precisely those for whom prolonged immobility carries the greatest risks: muscle weakness, blood clots, bone loss, and general deconditioning.
What This Means for Our Patients
This research confirms what we already practise at Melbourne Orthopaedic Group. Controlled loading of the ankle joint after replacement — the gentle stress of walking in a protected boot — stimulates bone and soft tissue recovery in a way that immobility cannot replicate. Earlier weight bearing helps the ankle regain motion, prevents scar tissue from stiffening the joint, and maintains muscle strength through the rehabilitation period.
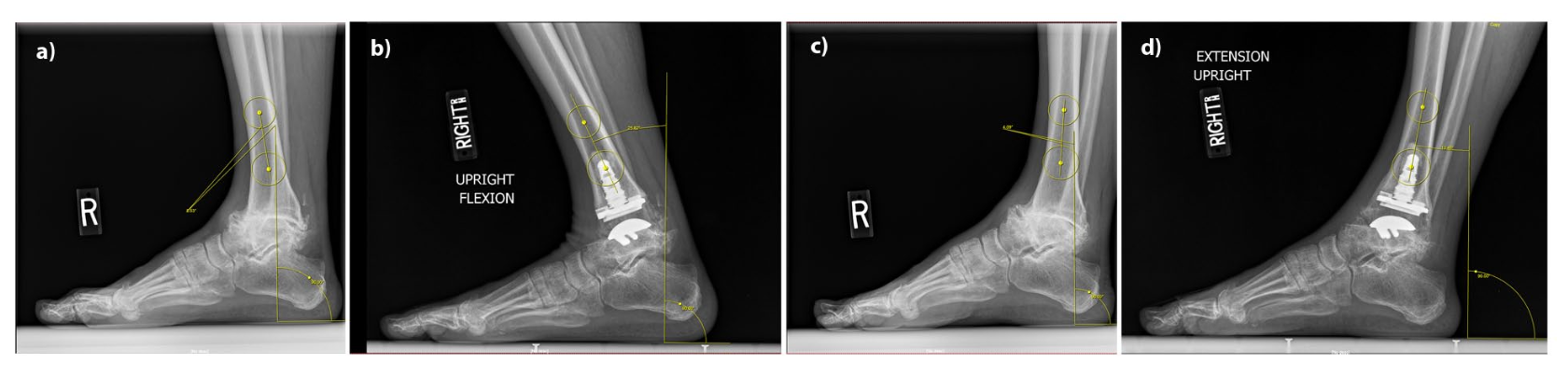
Xray measurement of (A) preoperative and (B) postoperative ankle dorsiflexion, and (C) preoperative and (D) postoperative ankle plantar flexion. Anatomic axis was approximated with a line connecting the centers of 2 circles in the tibial shaft.
Ankle dorsiflexion and plantarflexion was measured by the authors as an angle between this line and a line perpendicular (90 degrees) to the floor.
The early weight bearing (3 week group) had better range of motion after ankle replacement
The INBONE II implant’s robust modular stem fixation is particularly well suited to this approach, providing the initial stability needed to walk earlier without compromising implant security.
Listen to the Researchers
The March 2026 episode of the Foot & Ankle International Podcast features the journal editor and senior author discussing this paper at length — well worth a listen for anyone wanting to go deeper.
FAI March 2026 Podcast — Effect of Earlier Weightbearing After Total Ankle Arthroplasty
If you or a patient you are treating would like to discuss ankle arthritis or total ankle replacement, myself or my colleagues at Melbourne Orthopaedic Group would be happy to see you for a specialist assessment.
Book an appointment: (03) 9124 7960 | talia.admin@mog.com.au
Reference: Nguyen MT, Gross MM, Drake B, Choubey A, Weatherford BM. Effect of Earlier Weightbearing on Ankle Range of Motion and Complications After Primary Total Ankle Arthroplasty. Foot Ankle Int. 2026;47(3):281–290. doi:10.1177/10711007251401557