
Syndesmosis Injury (High Ankle Sprain): Symptoms, Diagnosis and Surgical Treatment
As the AFL, football, and netball seasons kick off, one injury reliably appears in the early rounds: the high ankle sprain, also called a syndesmosis injury. Unlike a common rolled ankle, a high ankle sprain involves the ligaments above the ankle joint — and it is an injury that is easy to miss on the sideline but can cause serious long-term problems if it is not treated correctly.
In this post I explain what a syndesmosis injury is, how it happens, how we diagnose it, and when surgery is needed — including surgical techniques I use regularly at my Melbourne foot and ankle practice: the AITFL internal brace and the syndesmotic tightrope.
What Is a Syndesmosis Injury (High Ankle Sprain)?
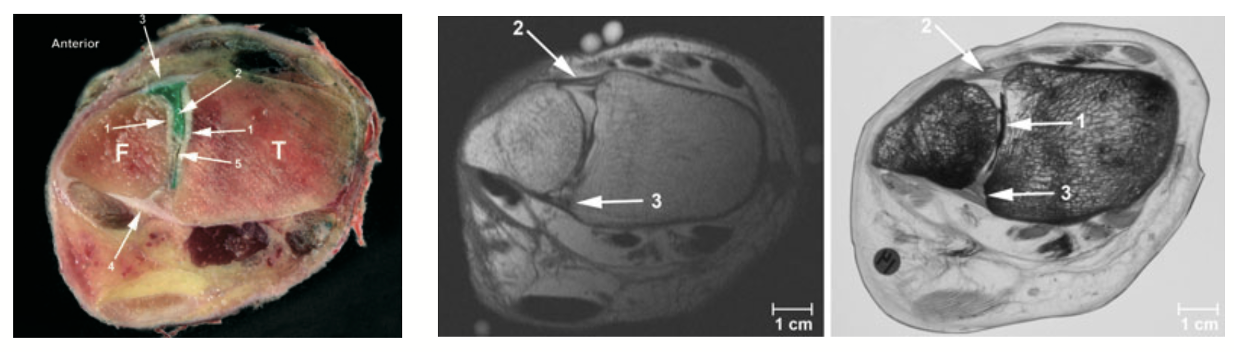
Just above your ankle, the two bones of your lower leg — the tibia (shin bone) and the fibula — are held together by a group of strong ligaments called the distal tibiofibular syndesmosis. Think of it as a clamp that keeps the ankle socket the correct width to cradle the dome of the ankle, talus bone snugly.
When these ligaments are torn — either partially or completely — the ankle socket can widen. An unstable syndesmosis puts abnormal stress on the ankle cartilage, which, if left untreated, can lead to early ankle arthritis, quite rapidly (1).
The ligament most commonly injured is the anterior inferior tibiofibular ligament (AITFL) — the ligament running across the front of the joint between the tibia and fibula. In more severe injuries, the deeper interosseous ligament (IOL) and the fibrous sheet running the length of the lower leg (the interosseous membrane) may also be disrupted.
How Does a High Ankle Sprain Happen?
Syndesmosis injuries are most common in contact and pivot sports — AFL, rugby, football (soccer), basketball, and netball. They usually happen in one of three ways:
• Foot planted and twisted outward (external rotation): The most common mechanism. The foot is flat on the ground and the body rotates over it — or a tackle forces the lower leg to twist outward over a fixed foot. This is the classic AFL or rugby injury.
• Ankle forced upward (hyperdorsiflexion): The foot is jammed upward toward the shin, such as when landing awkwardly from a jump. This can wedge the foot bone hard into the ankle socket and splay the syndesmosis apart.
• High-energy fractures: Several ankle fracture types — including the Maisonneuve fracture, where the fibula breaks near the knee — involve the syndesmosis. These can look deceptively normal on an ankle X-ray unless the full fibula is imaged.
One of the key dangers of a high ankle sprain is that it is often dismissed as a routine ankle sprain on the sideline. The athlete may walk away, only to find the ankle fails to settle over the following weeks (2).
Symptoms of a Syndesmosis Injury
Syndesmosis injuries feel different from a typical lateral ankle sprain. Key warning signs include:
• Pain above the ankle joint, between the tibia and fibula — not at the bony bump on the outside of the ankle
• Difficulty pushing off or walking up stairs, even with relatively mild swelling
• Tenderness along the front of the lower leg above the joint line
• Pain that seems out of proportion to how the ankle looks
• A feeling that the ankle is unstable or not quite right
If pain is sitting above the ankle joint rather than below it after a sporting injury, a specialist assessment is strongly recommended.
How Is a High Ankle Sprain Diagnosed?
Diagnosis combines clinical examination with imaging:
• Squeeze test and external rotation test: Simple bedside tests where compressing the calf or gently rotating the foot reproduces pain at the syndesmosis. These are useful screening tools in the clinic.
• Weight-bearing X-rays: The first investigation. We assess the gap between the tibia and fibula and the width of the ankle joint. Importantly, many syndesmosis injuries look normal on plain X-ray — a normal X-ray does not rule out the diagnosis and in fact plain X-rays do not form part of my assessment for syndesmotic injuries.
• MRI scan: The best investigation to confirm which ligaments are torn and grade the severity. MRI also detects cartilage injury inside the ankle joint, which is a recognised consequence of syndesmotic instability. The one problem with MRI scan is that it is not a dynamic (weight bearing) test, this is where WBCT comes in.
• Weight-bearing CT scan (WBCT): An advanced technique that images the ankle while you are standing on it. This is particularly useful for detecting subtle widening of the syndesmosis that a standard lying-down scan misses. I use this regularly in the borderline cases when the decision about surgery is not straightforward (3,4).
Syndesmosis Injury Treatment: Do I Need Surgery?
Not every syndesmosis injury requires surgery. Treatment depends on the severity:
• Mild (Grade I) — Stable: The ligament is stretched or partially torn but the ankle socket remains stable. A supportive boot and physiotherapy are usually sufficient, with return to sport in 4–8 weeks.
• Moderate (Grade II) — Latent instability: The AITFL is fully torn and subtle widening may only show on weight-bearing CT or stress imaging. Surgery is often recommended to prevent the ankle from progressively loosening.
• Severe (Grade III) — complete separation: The ligaments are completely disrupted and the ankle socket has visibly widened. Surgery is almost always required, and there is frequently an associated fracture.
Surgical Treatment: AITFL Internal Brace and Syndesmotic Tightrope
The goal of surgery is to restore the fibula to its correct position and hold it there while the torn ligaments heal. I use two procedures, most often in combination:
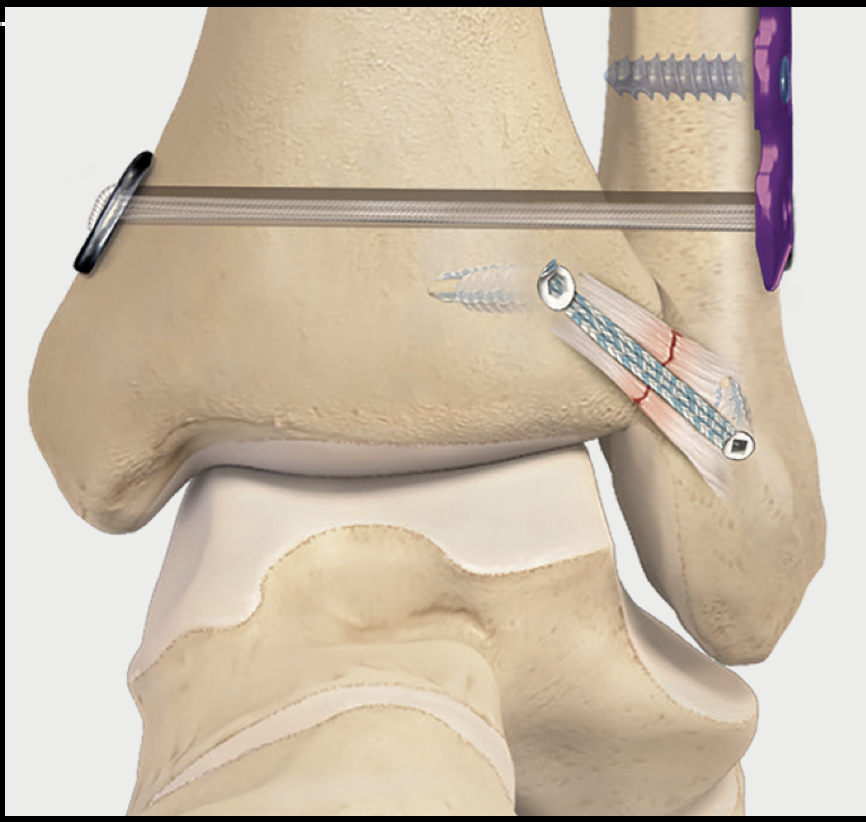
Fig 2. Diagram of AITFL internal brace and tightrope construct.
AITFL Internal Brace Reconstruction
The internal brace is a strong synthetic tape — roughly the thickness of a shoelace — anchored into the fibula and tibia at the exact position of the torn AITFL. It acts as an internal scaffold while the ligament heals, taking the load off the repair during early rehabilitation.
Where possible I also directly repair the torn AITFL underneath the tape — a repair-and-augment approach that gives the best healing result. The tape remains in place permanently and does not need to be removed routinely. This technique is well-suited to Grade I–II injuries and isolated AITFL tears (5,6).
Syndesmotic Tightrope Stabilisation
For moderate to severe injuries, a tightrope device provides more robust stabilisation across the full width of the joint. A small tunnel is drilled through both the fibula and tibia, and a strong suture tape is threaded through with small metal buttons on either side. When tensioned, it compresses the two bones back together, restoring normal joint width — like a zip tie pulling the bones into alignment.
Unlike metal screws that were used in the past, suture tape tightropes do not routinely need to be removed — they are flexible enough to allow the small natural movement at the syndesmosis without breaking (7).
In many patients with Grade II–III injuries I use both techniques together (8): an internal brace for the anterior ligament reconstruction and a tightrope for compression and rotational control. This combined approach provides robust early stability and supports a faster return to sport.

Fig 3. Intraoperative fluoroscopic images demonstrating a tightrope device reconstruction (top row) and then supplementation with the AITFL internal brace procedure (bottom row)
Recovery and Return to Sport After Syndesmosis Surgery
Modern constructs allow earlier weight-bearing than the metal screws used in the past. A general recovery framework:
• Weeks 0–2: Non-weight-bearing in a boot with the ankle elevated. Gentle toe and foot exercises.
• Weeks 2–6: Progressive weight-bearing. Physiotherapy begins — range of motion, early calf activation, balance training.
• Weeks 6–12: Transition to a lace-up brace. Walking normally, low-impact exercise, and sport-specific movement drills.
• 3–6 months: Most athletes with isolated syndesmosis injuries return to training around 3–4 months and full competition at 4–6 months. Complex fracture cases typically need closer to 6 months.
Summary
High ankle sprains (syndesmosis injuries) are common in contact and pivot sports and are frequently under-diagnosed in the early stages. The syndesmosis is the group of ligaments that holds the two lower leg bones together just above the ankle — when torn, the ankle socket can widen and become unstable, leading to accelerated cartilage wear. Diagnosis relies on clinical examination, MRI, and often weight-bearing CT. Milder injuries can be managed without surgery, but moderate to severe tears typically benefit from surgical stabilisation using AITFL internal brace reconstruction and/or tightrope fixation. With accurate technique and structured rehabilitation, most athletes make a full return to sport.
If you or a patient your are treating have concerns about a syndesmosis injury, I would be happy to see you for a specialist assessment on a timely basis.
Book an appointment: (03) 9124 7960 | talia.admin@mog.com.au
References
1. Waterman BR et al. Risk Factors for Syndesmotic and Medial Ankle Sprain. Am J Sports Med. 2011;39(5):992–998.
2. Williams GN et al. Syndesmotic Ankle Sprains in Athletes. Am J Sports Med. 2007;35(7):1197–1207.
3. Burssens A et al. Reliability and Correlation of Weight-Bearing CT With Clinical Assessment in Syndesmotic Ankle Injuries. Foot Ankle Int. 2018;39(2):166–175.
4. Sman AD et al. Diagnostic accuracy of clinical tests for ankle syndesmosis injury. Br J Sports Med. 2013;47(10):620–628.
5. Lubberts B et al. Arthroscopic diagnosis and treatment of syndesmotic injuries: a systematic review. Knee Surg Sports Traumatol Arthrosc. 2017;25(1):203–212.
6. Clanton TO et al. Biomechanical Comparison of Three Methods for Syndesmosis Repair in Rotation External Rotation Fractures. Foot Ankle Int. 2017;38(7):794–801.
7. Laflamme M et al. A Prospective Randomized Multicenter Trial of a Suture-Button versus a Syndesmotic Screw for Ankle Syndesmosis Injury. J Bone Joint Surg Am. 2015;97(7):559–566.
8.Lenz CG, Urbanschitz L, Shepherd DW. Dynamic syndesmotic stabilisation and reinforcement of the antero-inferior tibiofibular ligament with internal brace. Foot (Edinb) 2023; 56: 102026.